病人 BG > 500 mg/dL,可以 IV bolus RI 嗎?
情境:成人病人血糖檢測顯示 > 500 mg/dL。是否該開立 Regular insulin (RI) 固定劑量 IV bolus?
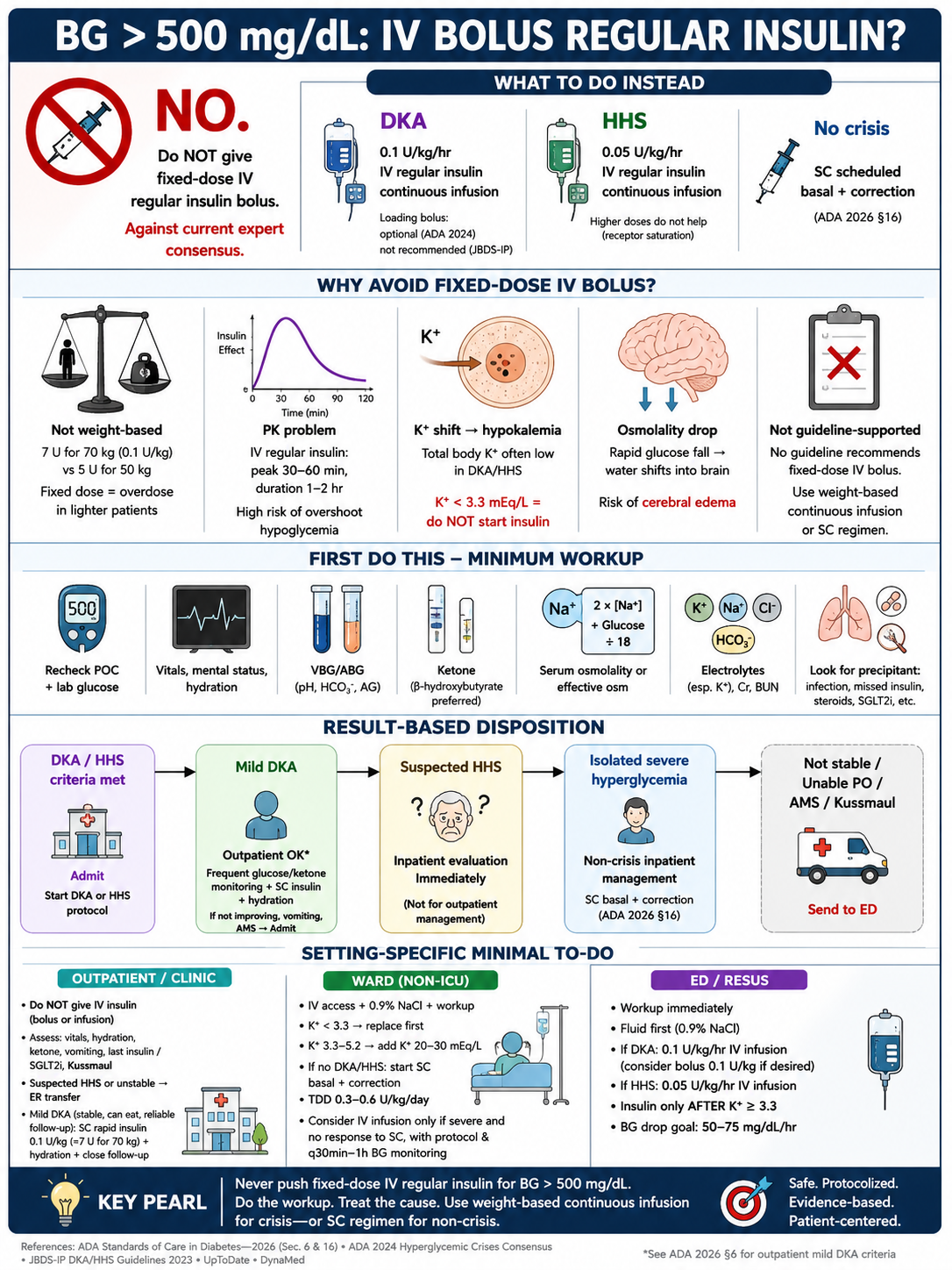
結論先給:不可以,違反當代專家共識。此答案不分病人是否符合 DKA / HHS 標準 — 即便確認為危象,ADA 2024 Hyperglycemic Crises Consensus 與 JBDS-IP DKA 2023 之處置流程均為 0.1 U/kg/hr continuous IV infusion,loading bolus 在 ADA 2024 列為可選、在 JBDS-IP 明確不建議、在 HHS 因 receptor saturation 直接不打;任何不依權重計算之固定劑量 IV bolus 在現行指引都找不到根據。本文依「門診 / 病房 / 急診」三情境列最低限度處置,並補上 1970 年代 high-dose insulin era 之歷史脈絡。
結論(不分有無 DKA / HHS)
- 單純嚴重高血糖(未達 DKA / HHS 標準):固定劑量 IV bolus 不可。正確處置 = SC scheduled basal + correction(ADA 2026 §16)。
- 確認 DKA:固定劑量 IV bolus 不可(flat dose 不分權重,任意固定值均偏離 0.1 U/kg 標準)。正確處置 = 0.1 U/kg/hr continuous IV infusion;loading bolus 在 ADA 2024 列為可選、JBDS-IP 明確不建議。
- 確認 HHS:固定劑量 IV bolus 不可。正確處置 = 先補液;0.05 U/kg/hr continuous IV infusion(HHS-predominant),加量無加成(receptor saturation)。
固定劑量 IV bolus 屬 supra-physiological 處方範式:70 kg 病人之危象 bolus 標準為 0.1 U/kg ≈ 7 U,任何不依權重計算之固定值容易超標,體重愈輕、超標愈嚴重。風險包含反彈性低血糖、insulin 驅動之低血鉀、滲透壓快速下降之 cerebral edema;IV regular insulin 藥動學在 60 min 內幾乎全數發揮,bedside 監測跟不上。「下一步」永遠是:最低限度評估 → 依檢驗結果分流 → SC scheduled insulin(非危象)或 protocol-driven IV continuous infusion(危象),絕不是一次推注固定劑量。
為什麼一定要先做評估(即便「看起來不像」)
「無 DKA/HHS 明顯表徵」不等於排除。容易漏診的情境:
- 老年或失智病人 HHS:初期意識變化容易被歸因於「平常糊塗」,但 effective osmolality > 320 mOsm/kg 已達 HHS 標準。
- POC 誤差或 IV line 污染取血:見到 BG 500+ 而病人狀態完全不對盤時,先重驗。
最低限度評估(門診 / 病房 / 急診 通用)
- 重測 POC + 中央實驗室血糖:排除 POC 誤差、檢體標籤錯置、IV-line 污染(從點滴含葡萄糖端取血最常見)。
- 意識(GCS)、生命徵象、容積評估:排除意識變化、容積不足、休克。
- VBG / ABG(pH、HCO₃⁻、anion gap):DKA 標準 = pH < 7.3、HCO₃⁻ < 18、AG > 10。
- Ketone(serum β-hydroxybutyrate 優於尿液 ketone strip):DKA 必要;SGLT2i 使用者尤其需要。
- 血清滲透壓 或 effective osm = 2 × [Na⁺] + glucose ÷ 18:HHS 標準 = effective osm > 320 mOsm/kg。
- 電解質(K⁺、Na⁺、Cl⁻、HCO₃⁻)、Cr、BUN:K⁺ 是 insulin 啟動的閘門。
- 找誘發因子:UA、CXR、培養(疑感染)、藥物史(漏打、新增類固醇、SGLT2i、antipsychotic、ICI)— 處置根因。
結果分流
- 符合 DKA / HHS 標準 → 立刻進入該院 DKA 或 HHS 處置流程(ADA 2026 §16 / ADA 2024 Hyperglycemic Crises Consensus / JBDS-IP),不在本文範圍。
- 輕度 DKA(血液動力學穩定、意識清楚、可口服、可 SC 給藥)→ ADA 2026 §6 明文:可以「頻繁監測血糖與 ketone、無熱量補水、SC insulin」處置;嘔吐、意識變化、酮體或血糖未隨 insulin 改善 → 立刻轉住院。
- 疑似 HHS → ADA 2026 §6 明文:立刻住院評估治療,不適合門診觀察。
- 單純嚴重高血糖(無 acidosis、無 ketosis、意識清楚、容積尚可、無 hyperosmolar)→ 走住院非危象高血糖之處置路線(ADA 2026 §16)。
為什麼固定劑量 IV bolus 不適當
不分是否為危象,固定劑量 IV bolus 都不對:
- 不依權重計算。flat dose 不考慮體重。ADA 2024 / JBDS-IP 之危象 bolus 上限為 0.1 U/kg(70 kg ≈ 7 U、50 kg ≈ 5 U),且當代處置流程多已捨棄 loading bolus,改為直接 0.1–0.14 U/kg/hr continuous infusion。任何不依權重之固定值與此標準無對應關係;體重愈輕之病人,固定劑量相對偏離愈大。
- 藥動學不利。IV regular insulin t½ ≈ 5–10 min、peak 30–60 min、duration 1–2 hr。一次推注之固定劑量在 60 min 內幾乎全數發揮 → 反彈性低血糖機率高,且 bedside POC q30 min 監測通常跟不上。
- K⁺ shift。每 U insulin 將細胞外 K⁺ 推向細胞內;DKA/HHS 病人 total body K⁺ 通常已耗竭,固定劑量 IV bolus 之低血鉀風險與劑量呈正相關,可誘發 arrhythmia。K⁺ < 3.3 mEq/L 是啟動 insulin 之禁忌(ADA 2024 Hyperglycemic Crises Consensus 與 JBDS-IP DKA 2023 共識;先補 K⁺ 至 ≥ 3.3;UpToDate DKA Tx 採更保守的 K⁺ ≥ 3.5 mEq/L 門檻、同此精神)。
- 滲透壓快速下降 → cerebral edema 風險。BG > 500 對應 effective osmolality 顯著升高(葡萄糖貢獻之滲透壓 ≈ glucose ÷ 18);快速降糖會把血漿水分推進腦細胞。兒科 DKA 的 cerebral edema 證據明確;成人 HHS 亦有記載。目標降糖速率為 50–75 mg/dL/hr(不是「越快越好」)。
- 違反專家共識:沒有指引把固定劑量 IV bolus 寫進處方。ADA 2026 §16 通篇講 weight-based 每日總劑量(0.3–0.6 U/kg/day)、scheduled basal + prandial + correction SC、IV insulin 僅 在 critical care 採 continuous infusion + 院內 validated 處置流程,完全沒有推注 bolus 之寫法。ADA 2024 Hyperglycemic Crises Consensus 與 JBDS-IP HHS 對 HHS 採 0.05 U/kg/hr 之原理為 insulin receptor 在 low dose 已飽和、加量無顯著額外降糖。
三情境最低限度處置
門診
門診沒有 IV insulin titration、hourly POC、護理人力做 K⁺ 補充的條件。
- 不要在門診開 IV insulin(無論 bolus 或 infusion)。固定劑量 IV bolus 在門診屬高風險處方。
- 評估血液動力學、意識、容積狀態、ketone(若有尿液 ketone strip)、嘔吐、Kussmaul breathing、口渴 / 多尿病史、上一次胰島素 / SGLT2i 服用時間。
- 疑似 HHS、無法口服、意識變化、Kussmaul、嘔吐、持續漏打 → 立刻急診轉送(救護車,不要病人自駕)。等候期間建立 IV access、0.9% NaCl 500 mL 慢滴、finger BG q30 min 紀錄。
- 輕度 DKA(血液動力學穩定、意識清楚、可口服、可 SC 給藥、有家屬監督):ADA 2026 §6 允許門診處置 = 頻繁監測血糖與尿液 / 血液 ketone、無熱量補水、SC rapid-acting insulin(lispro / aspart 0.1 U/kg SC ≈ 7 U for 70 kg),並安排 24 h 內內分泌 / 急診追蹤;但 ketone 或血糖未改善、嘔吐、意識變化、病情惡化 → 立刻急診。
- 單純嚴重高血糖(檢驗暫時做不到,但臨床無危象跡象):仍建議當天急診完成評估,不要單純門診觀察。
病房(一般病房)
- 立刻停掉固定劑量 IV bolus 醫囑;改為建立 IV access + 0.9% NaCl + 最低限度評估(同上)。
- K⁺ < 3.3 mEq/L → 暫停 insulin,先補 KCl 至 K⁺ ≥ 3.3。
- K⁺ 3.3–5.2 → IV fluid 同時加 K⁺ 20–30 mEq/L。
- 檢驗確認為 單純嚴重高血糖(未達 DKA/HHS 標準):
- 起始 SC 對策(ADA 2026 §16):scheduled basal(glargine / detemir / degludec)+ correction SC rapid-acting per correction scale。
- 依體重之 TDD 0.3–0.6 U/kg/day 起始;correction 從 140–150 mg/dL 起始。
- 第 1 型糖尿病必須 basal + correction;ADA 2026 §16.10 明指單獨 sliding scale 不被推薦。
- 嚴重高血糖(> 300–350 mg/dL)且 SC rapid-acting 數小時無效:可考慮短期 IV insulin infusion,但前提是護理可 q30 min – q1 h fingerstick + 有院內 validated 處置流程(ADA 2026 §16.2、§16.8a)。一般病房通常做不到 → 轉 ICU / step-down 較安全。
- 檢驗顯示 達 DKA / HHS 標準 → 轉 ICU + 走院內 DKA / HHS 處置流程。
- 同步處理誘發因子:感染、漏打、類固醇、新增 SGLT2i、新發糖尿病、心血管事件、stroke。
急診
- 立刻停掉固定劑量 IV bolus 醫囑。
- ABC、IV access ×2 large-bore、O₂ / monitor。
- 一次抽:BG、CBC、CMP(K⁺、Na⁺、Cl⁻、HCO₃⁻、Cr、BUN)、β-OHB、滲透壓、ABG / VBG、UA、lactate、感染相關(CXR、UA 培養、發燒時血液培養)。
- 先補液:0.9% NaCl 1–1.5 L 在第一小時(15–20 mL/kg),重評容積、corrected Na⁺;HHS 病人脫水更重,後續液體種類依 corrected Na⁺ 與血液動力學調整。
- K⁺ 結果出來:< 3.3 → 暫停 insulin、先補 K⁺;3.3–5.2 → fluid 加 K⁺ 20–30 mEq/L;> 5.2 → 暫不補 K⁺ 但可給 insulin。
- Insulin(待第一袋 fluid 完、K⁺ ≥ 3.3 之後):DKA / HHS 處置流程 = 0.1 U/kg/hr continuous IV infusion(HHS-predominant 可降至 0.05 U/kg/hr,因 receptor saturation 加量無益)。可選 bolus 0.1 U/kg 一次(當代處置流程多省略)。從來不會是一次推注固定劑量。
- 目標降糖速率 50–75 mg/dL/hr,避免 cerebral edema。BG ≤ 250 mg/dL → 點滴改 D5W / D5½NS、insulin 降至 0.02–0.05 U/kg/hr 維持。
- 處理誘發因子(最常見:感染、漏打、新發第 1 型糖尿病、SGLT2i 相關 DKA、心肌梗塞、stroke、antipsychotic / ICI / 糖皮質類固醇新增)。
固定劑量 IV bolus 的歷史脈絡(1973 前之高劑量時代與 1973–1976 典範轉移)
「固定劑量 IV bolus」此一處方範式並非憑空產生;它是 1973 年以前 conventional high-dose insulin therapy era 的殘影。
1940s – 1973:conventional / high-dose era
從 1940 年代到 1970 年代初期,DKA 治療的主流假設是「酮酸中毒病人有顯著 insulin resistance、需大劑量克服」。當時公認的劑量範圍:
- Howard Root(Boston, 1945)系列:第一個 3 h 平均約 83 U insulin、24 h 累積平均 287 U(range 50–1770 U),混合 IV bolus + SC + IM 給藥。
- Birmingham(UK)系列:意識昏迷者 24 h 累積可達 500–1400 U。
- 1960–70 年代內科教科書多列「first hour 50–100 U insulin」之 IV bolus / IM 起始建議。
現行的固定劑量 IV bolus 處方位於此 1973 前連續譜的下緣,不曾是被命名的標準推薦,只是該年代「打大劑量」氛圍下的延續切片;具體固定劑量數值在當代證據框架下並無試驗支持之區別。
1973 – 1976:low-dose 典範轉移
三篇 landmark RCT 推翻了 high-dose 假設,證實 low-dose continuous IM / IV insulin(5–10 U/hr,約 0.1 U/kg/hr) 與 high-dose 同樣降糖、卻顯著減少低血糖與低血鉀:
- Alberti KG, Hockaday TD, Turner RC. Small doses of intramuscular insulin in the treatment of diabetic “coma”. Lancet 1973;2(7828):515–22.
- Page MM, Alberti KG, Greenwood R, et al. Treatment of diabetic coma with continuous low-dose infusion of insulin. BMJ 1974;2(5921):687–90.
- Kitabchi AE, Ayyagari V, Guerra SM. The efficacy of low-dose versus conventional therapy of insulin for treatment of diabetic ketoacidosis. Ann Intern Med 1976;84(6):633–8.
這三篇之後,當時主導的指引組織 — ADA(1980 年代開始持續更新 DKA / HHS 章節)、JBDS-IP(2010 年代起 UK 端正式 protocol 化)、EASD — 之 DKA / HHS / 住院高血糖章節從未再出現「固定劑量 IV bolus」這個處方;之後 1990 年代興起的臨床決策資料庫(UpToDate、DynaMed)亦完全沿用此 low-dose 架構。當代處置流程改為 0.1 U/kg/hr continuous IV infusion ± 可選之 0.1 U/kg bolus,且 ADA 2024 / JBDS-IP 多省略 loading bolus。
現代任何 evidence-based 處方體系都不支持以固定劑量 IV bolus 治療高血糖;遇到此處方,應視為歷史殘存、依當前處置流程重寫。
唯一現代仍會用 bolus RI 的情境:急性高血鉀
值得區分的例外:急性高血鉀(K⁺ ≥ 6.0–6.5 mEq/L)需要 transient K⁺ cellular shift 時,當代指引仍明確使用 IV soluble insulin 10 U + 25 g dextrose 一次推注(UKKA 2023 Grade 1B;DynaMed Hyperkalemia in Adults;KDIGO 同此架構);機轉為 insulin 透過 Na⁺/K⁺-ATPase 把細胞外 K⁺ 推入細胞,30–60 min 內血鉀下降約 0.6–1.2 mEq/L;同時 25 g dextrose 預防低血糖(若 BG < 126 mg/dL 事後再 10% glucose 50 mL/hr × 5 h)。
跟前文嚴重高血糖場景目的相反:
| 情境 | K⁺ shift 角色 | Insulin 劑量範式 |
|---|---|---|
| 嚴重高血糖(DKA / HHS) | total body K⁺ 已耗竭,shift = harm | 0.1 U/kg/hr continuous infusion;K⁺ < 3.3 為禁忌 |
| 急性高血鉀 | K⁺ 過多,shift = 治療目標 | 10 U IV fixed + dextrose 一次推注 ✓ |
不要把這個 cellular-shift 適應症誤用於高血糖。10 U IV + 25 g dextrose 是針對 transient K⁺ shift 被證據驗證之安全劑量、且必與 dextrose 同打;用於降血糖之固定劑量 IV bolus 不論哪個情境都不在 guideline。
文獻參考
-
[L4 guideline] American Diabetes Association Professional Practice Committee. 16. Diabetes Care in the Hospital: Standards of Care in Diabetes—2026. Diabetes Care 2026;49(Suppl 1):S339–S355. DOI 10.2337/dc26-S016
引用主張:Inpatient hyperglycemia 之 SC basal + prandial + correction framework;IV infusion 限 critical care + validated protocol;TDD 0.3–0.6 U/kg/day;correction 起始 140–150 mg/dL;單獨 sliding scale 不推薦;無 IV bolus 寫法。 -
[L4 guideline] American Diabetes Association Professional Practice Committee. 6. Glycemic Goals, Hypoglycemia, and Hyperglycemic Crises: Standards of Care in Diabetes—2026. Diabetes Care 2026;49(Suppl 1):S132–S149. DOI 10.2337/dc26-S006
引用主張:Hyperglycemic crisis risk factors(SGLT2i、glucocorticoid、antipsychotic、ICI);mild DKA outpatient self-management criteria;suspected HHS 須 inpatient。 -
[L4 consensus] Umpierrez GE, Davis GM, ElSayed NA, et al. Hyperglycemic Crises in Adults With Diabetes: A Consensus Report. Diabetes Care 2024. DOI 10.2337/dci24-0032 · PMID 39052901
引用主張:2024 成人 DKA / HHS / mixed crisis consensus;continuous IV infusion 0.1 U/kg/hr (DKA)、0.05 U/kg/hr (HHS);K⁺ < 3.3 gating;no-bolus modern protocol。 -
[L4 guideline] Joint British Diabetes Societies for Inpatient Care. The Management of Diabetic Ketoacidosis in Adults. 2023 update. PMID 37537152
引用主張:UK FRII (fixed-rate IV insulin infusion) 0.1 U/kg/hr、K⁺ gating、no loading bolus。 -
[L4 guideline] Joint British Diabetes Societies for Inpatient Care. The Management of the Hyperosmolar Hyperglycaemic State in Adults with Diabetes. 2022 update.
引用主張:UK HHS fluid first;後續低劑量 insulin(0.05 U/kg/hr,視 3-β-OHB 而定)。 -
[L5 system] UpToDate. “Glycemic management in hospitalized adults with diabetes mellitus.” Topic 1770 Version 49.0. Updated Apr 27, 2026. Wolters Kluwer Health. Accessed 2026-05-15.
引用主張:Inpatient non-crisis:BG ≥ 200 → scheduled SC insulin;BG > 300–350 + SC 失敗 → 短期 IV infusion(限 ICU / step-down + frequent fingerstick);無 IV bolus 寫法 — supporting echo of ADA consensus。 -
[L5 system] UpToDate. “Diabetic ketoacidosis in adults: Treatment.” Topic 1795 Version 63.0. Updated Feb 11, 2026.
引用主張:Adult DKA low-dose IV insulin、continuous infusion 0.1 U/kg/hr 為標準;K⁺ ≥ 3.5 mEq/L 為更保守啟動門檻 — supporting echo of ADA / JBDS consensus。 -
[L5 system] UpToDate. “Hyperosmolar hyperglycemic state in adults: Treatment.” Topic 143587 Version 2.0. Updated Nov 25, 2024.
引用主張:HHS fluid first;0.05 U/kg/hr insulin;higher doses 無加成(“insulin receptors are fully saturated by the lower doses”,原文 quoted in body)— supporting echo of ADA / JBDS receptor-saturation rationale。 -
[L5 system] DynaMed. “Glucose Control in Critical Care Patients With and Without Diabetes.” EBSCO. Updated Apr 9, 2026. Accessed 2026-05-15.
引用主張:ICU validated IV insulin protocol;target 140–180 mg/dL;protocol-driven continuous infusion 為唯一 IV insulin 寫法。 -
[L1 landmark RCT] Alberti KG, Hockaday TD, Turner RC. Small doses of intramuscular insulin in the treatment of diabetic “coma”. Lancet 1973;2(7828):515–22. DOI 10.1016/s0140-6736(73)92346-5
引用主張:1973 RCT — 5 U/hr IM regular insulin 與 high-dose 同效、hypoglycemia / hypokalemia 顯著降低;終結 pre-1973 high-dose era。 -
[L1 landmark RCT] Page MM, Alberti KG, Greenwood R, et al. Treatment of diabetic coma with continuous low-dose infusion of insulin. BMJ 1974;2(5921):687–90. DOI 10.1136/bmj.2.5921.687
引用主張:1974 RCT — continuous IV insulin infusion 取代 IM 路徑,成為現代 protocol 雛形。 -
[L1 landmark RCT] Kitabchi AE, Ayyagari V, Guerra SM. The efficacy of low-dose versus conventional therapy of insulin for treatment of diabetic ketoacidosis. Ann Intern Med 1976;84(6):633–8. DOI 10.7326/0003-4819-84-6-633
引用主張:1976 直接比對 low-dose vs conventional high-dose — 同效但低併發症;ADA 後續以此為 evidence base 採用 0.1 U/kg/hr framework。
文獻層級說明
本文採用 EBM-CC 6S Haynes pyramid 標註引用層級:
- L1 Studies:原始研究(RCT、cohort)
- L2 Syntheses:systematic review、meta-analysis、journal-curated review
- L3 Synopses of syntheses:ACP Journal Club、DARE
- L4 Summaries:guideline、教科書 chapter
- L5 Systems:UpToDate、DynaMed、BMJ Best Practice 等 point-of-care CDSS
L4 與 L5 皆為 peer-reviewed structured expert opinion;本文採 tier-honest 引用,每筆參考明示 tier,避免假裝在做原始文獻評閱。
引用態度:
- L4 ADA 2024 Hyperglycemic Crises Consensus + JBDS-IP DKA/HHS 為 navigator-cited via OpenEvidence + Gemini grounded search;本文僅引用 guideline-level 框架主張(dose-rate framework、K⁺ gatekeeping、no-bolus modern protocol),未引用任何 primary RCT 之具體數值。
- L5(UpToDate × 3、DynaMed × 1)為 2026-05-15 透過 mbp / hm4 Chrome Beta + sub-utd / sub-dynamed CLI 即時擷取至 wiki_raw 之 snapshot,PG-registered 並標記
cite_directly=false;本文將其作為 consensus 的 supporting echo,主張仍以 L4 為原始來源。 - L1 #10–12 三篇 1973–1976 landmark papers 為 navigator-cited via UpToDate DKA Tx 章節 + ADA 2024 consensus 之 reference list;本文僅引用「low-dose 同效 + 更安全」之質性 finding,未複述各 RCT 之具體 numeric outcome(per Law §citation hygiene:未直接 fetch primary full text 者不引用 trial-specific values)。
- OpenEvidence 因無 peer review、6S blank(純 LLM aggregator),不列入引用表,僅作為 navigator 線索(surface ADA 2024 + JBDS-IP + Karslioglu French BMJ 2019 等資料)。
- 本文涵蓋成人。兒童 DKA「絕對不打 insulin bolus」之 cerebral edema 風險另論,請參考 ISPAD 2022 與 ADA 2026 §15。